



How we can help your Psoriasis
At DigiDerm we know how frustrating it is to suffer with skin conditions and how easy it is to get lost in all the information out there on the internet. We’ve put together this guide to give you all you need to know about psoriasis and most importantly how you can manage your psoriasis, and get back to doing the things you love, without it getting in the way!
DigiDerm is run by practicing NHS clinicians and we pride ourselves on providing you the best evidence based care. If you know what you need you can go straight to our treatments and select the treatment you want.
If you’re not sure what you need then we’ve put together some info below to help you find out more about psoriasis and what treatment is right for you. If you’re still not sure at the end then don’t hesitate to book a telephone or video consultation with one of our clinicians. We would be happy to help with any questions and if we can’t help, you won’t pay a penny. We’ll follow you up to check everything’s working as it should be and make sure you get the right treatments for your psoriasis.
Make sure to check out our FAQs section below, which has some of the most common questions we get about psoriasis.
Psoriasis is a fairly common inflammatory condition of the skin affecting around 3% of the population. Recent research suggests that psoriasis is likely an autoimmune disease. This is a condition where the body’s own immune system attacks itself.
Psoriasis can start at any age but is most likely to present between the ages of 20 and 30 or 50 and 60. It can affect anyone and is equally likely to affect men and women but is more common amongst white people and less common amongst the Asian, black and Hispanic races. It tends to present as red and inflamed scaly plaques and most commonly appears on extensor areas of the skin. This means the areas of the skin that bend such as the front of the knees or backs of the elbows and can also commonly occur on the scalp. Whilst these are the most common presentations of psoriasis, symptoms can also be widespread covering large areas of the body.
Is Psoriasis linked to arthritis?
Put simply yes. This condition is commonly associated with a particular form of arthritis called psoriatic arthritis and studies suggest that up to 30% of people with psoriasis could have this form of arthritis.
Is psoriasis linked to Heart Disease?
Sadly this is another yes. Studies suggest a strong link between psoriasis and heart disease, although this is more common in people that have severe psoriasis. It is important to report any potential heart issues to your GP and even more important if you have psoriasis. Your GP will likely have a lower threshold for referring you for further tests. Potential signs of heart disease include: chest pain, shortness of breath, dizziness, blackouts, palpitations (feeling your heart flutter in your chest), etc.
If you have had any of the above symptoms we recommend contacting your GP for further advice.
Is Psoriasis Genetic?
There is thought to be a very strong link with genetics and the cause of psoriasis. Of the people that develop psoriasis, 40-50% of them are estimated to have another family member that suffers with the condition. This is even more likely to be the case if you first developed psoriasis before the age of 20.
What Triggers Psoriasis?
Stress is a well-documented trigger for psoriasis flares. If you are struggling with your stress levels then this is something worth looking at to get your psoriasis under control. At DigiDerm we understand how important stress and mental health are when it comes to skin conditions, so check out our mental health page for more information and resources that can help you.
Sunlight: Most people will find sunlight beneficial to their psoriasis and will actually find exposure to sunlight will settle their psoriasis however in a smaller number of people sunlight can make their condition worse.
Smoking is generally terrible for your health and so if you needed another reason to quit it’s also known to cause and worsen psoriasis. Not to mention it increases your risk of heart disease which having psoriasis already does. Stopping smoking is very difficult but with the right help it is absolutely possible. Talk to your local Chemist about how they can help you with this.
Trauma: Sometimes psoriasis can occur at the site of an injury to your skin. This is known as Koebner Phenomenon.
Drugs: A number of medications have been linked with psoriasis. Some of the most common examples include but are not limited to: lithium, imiquimod, terbinafine, beta blockers and drugs to treat malaria such as chloroquine.
If you think one of your medications has caused psoriasis, it is important you do not stop taking them but to speak to your GP or whoever prescribes it to you for more advice.
Pregnancy: Many women will find that their psoriasis actually improves during pregnancy. It can however get worse after giving birth.
Alcohol: Heavy drinking has been linked with psoriasis and it is thought that alcohol may have a direct impact in worsening psoriasis. If you feel you need help with cutting back on drinking then contact your GP or local drug and alcohol service.
Streptococcal infections: Streptococcus is a type of bacteria commonly associated with tonsillitis (Infection of the tonsils). Infections with this bacteria particularly of the throat are known to provoke a specific type of psoriasis known as guttate psoriasis. Guttate psoriasis causes small (generally less than 1cm) sores to appear often covering a large area of the body including the chest, arms, legs and scalp.
HIV: It’s important to be aware that severe or treatment resistant psoriasis has been identified as a recognised potential indicator of HIV and can be the first sign in some patients. If you think this is a possibility then its best to speak to your local sexual health clinic who can help you with getting tested and ruling this out.
There are different types of psoriasis and it can appear in a variety of circumstances or areas, so the symptoms may differ depending on the type of psoriasis you are experiencing.
We will cover the most common types in this guide but there are some rarer forms as well. The main types of psoriasis are listed below with example images to demonstrate how it can present.

Plaque Psoriasis
This is the most common type of psoriasis and of the people that develop psoriasis 80-90% develop this type. Dry and scaly skin lesions known as plaques develop on the skin. These lesions can appear anywhere on the body but are most common on the elbows, knees, scalp and lower back. The plaques can be itchy and painful.

Scalp Psoriasis
This is a type of plaque psoriasis as mentioned above. It can appear in parts or over the whole scalp. Some people find it very itchy whilst others will experience no discomfort.

Nail Psoriasis
Nails are affected in around half of all people that suffer with psoriasis. It can cause the nails to develop dents or become discoloured. In some circumstances it can even cause nails to crumble or separate from the nail bed. You can use the same creams to treat nail psoriasis as with other forms of psoriasis however you may need to treat these longer than a flare on the skin, as nails can be difficult to treat. If using steroid creams potent or very potent steroids tend to be better suited for nail psoriasis. See our steroid guide for more info.
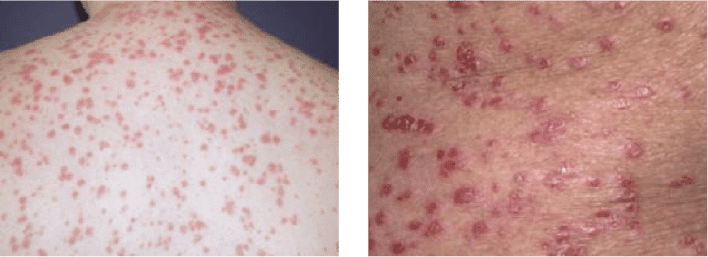
Guttate Psoriasis
This type of psoriasis has been shown to occur more commonly after sore throat infections caused by the bacteria streptococcus. It presents as small (less than 1cm) sores over large portions of the body, often including the chest, arms, legs and scalp. This condition is more likely to occur in younger people such as children and teenagers.
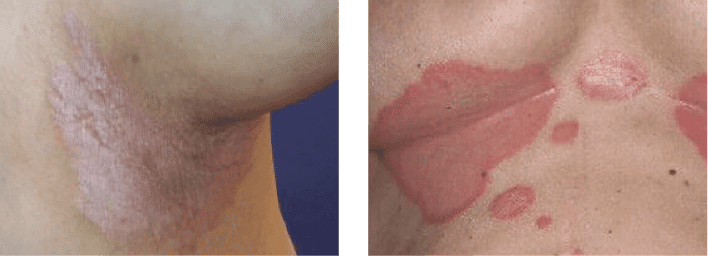
Inverse (Flexural) Psoriasis
This type of psoriasis effects the folds in the skin and areas of skin that regularly rub together. This is most likely to occur in the armpits, between the buttocks, under the breasts and around the groin. These are also common locations for eczema to occur so it is important to consider this and get a diagnosis from a healthcare professional before starting treatment.
Psoriasis is generally not too difficult for a clinician to diagnose. It has some typical features generally including red, inflamed, dry skin with a fairly characteristic silvery scale in most cases.
Whilst it is generally straight forward it can at times be unclear if its psoriasis or another skin condition, so if you are in any doubt after looking at the pictures above, please don’t hesitate to book for a telephone or video consultation with one of our dermatology Pharmacists and we’ll be more than happy to help you figure it out. Click here to make appointment
NOTE: Don’t worry if you are unsure of what treatments to select. You can start a simple online questionnaire-based consultation, attach some photos, and we will let you know if the treatment you have selected is safe and appropriate- if not, we will recommend an alternative. If you’d prefer to talk over the phone, you can book in for a telephone or video consultation with one of our friendly dermatology specialists and we can recommend suitable treatments and advice.
Here we will discuss some of the treatment choices that we offer for psoriasis in line with the latest clinical guidelines for dermatology in the UK. We will also discuss some alternative treatments towards the end that we don’t currently offer but are interesting to learn about (click on the products for more information and to start a consultation).
We will start with steroids. These are to be used when you have a flare of psoriasis. Make sure to apply them sparingly and usually for no longer than 7 days continuously unless advised by a clinician. They are a great way to settle down a flare of psoriasis but not a long term solution.
There are varying strengths of steroids from mild to very potent. If you already know what strength you need, as you’ve had it before, this is likely to work for you again. If you have not tried steroid creams before it is worth being cautious and starting with a milder steroid, only using potent steroids on the advice of a clinician.
You should be particularly careful when applying steroid creams to sensitive skin areas such as your face. You shouldn’t apply steroids to the face unless advised to do so by a clinician after assessment and you should never use anything more than moderate strength steroids in this area.
We are happy to have a look at some pictures or speak on a video or telephone call to advise on what strength we think you need if you’re unsure. Click here to book an appointment
Steroid Cream Guide
Mild Steroid Creams:
e.g- Hydrocortisone 1.0% ointment/cream
(Can be applied to the face on advice of a clinician)
Moderate Steroid Creams:
e.g- Eumovate (clobetasone butyrate 0.05%) cream and Betnovate RD (betamethasone valerate 0.025%)
(Can be applied to the face or genitals on advice of a clinician)
Potent Steroid Creams:
e.g- Betnovate (betamethasone valerate 0.1%)
Combination products with vitamin D analogues (psoriasis only):
– Dovobet (betamethasone dipropionate 0.05% with calcipotriol 50mcgs/g)
– Enstilar (betamethasone dipropionate 0.05% with calcipotriol 50mcgs/g)
Do NOT apply to the face or genitals.
Very Potent Steroid Creams:
e.g- Dermovate (clobetasol propionate 0.05%)
Do NOT apply to the face or genitals.
Vitamin D Analogues
Vitamin D analogues have been shown to be very effective in treating psoriasis flares. These provide a potential alternative to steroids so are particularly useful if you struggle with side effects when using steroids such as skin thinning or staining. They can also be used long term if needed whilst steroids can only be used for limited courses.
Two examples of these creams include:
Dovonex (calcipotriol) Ointment: This can be used for psoriasis flares although should not be used on the face or genitals, as it can cause irritation.
Silkis (calcitriol) ointment: This has a similar effect to the above ointment however has the added benefit of being suitable for use on the genitals or face. For this reason the ointment is particularly useful for flares in these areas where potent steroid creams would be inappropriate.
In addition to products containing vitamin D analogues alone, we also offer combination products that also contain a steroid. These are particularly useful in difficult to treat psoriasis or where the individual products alone have not cleared the flare.
Examples of such products include:
Dovobet ointment/gel or Enstilar foam (calcipotriol and betamethasone).
Both of these products contain a strong steroid as well as a vitamin D analogue and for this reason attack the psoriasis flare in two separate ways.
Enstilar is particularly useful if your psoriasis covers a large area, as it comes as a foam spray making it easier to apply over a large area more quickly.
Emollients
The other major component of most psoriasis treatment is finding the right emollient for you. Emollients form a protective barrier on the skin and block moisture from escaping. This prevents the skin from drying out and makes it less likely to become irritated and inflamed, as can often happen in psoriasis.
It is important to apply plenty of emollient and to do so regularly. Thicker ointments last for around 12 hours whilst creams, lotions and gels only tend to last around 8 hours, meaning you would need to apply these thinner preparations at least three times a day and ointment twice a day for optimal results.
Ointments are better at locking in moisture because they are thicker and more oily however because of their oily texture some people don’t like applying these as much, as they can remain visible on the skin for longer after being applied and can stick to clothing and bedding, etc. Creams, lotions and gels are generally better tolerated due to them being thinner and thus more easily absorbed by the skin but because of this they will not moisturise the skin as affectively as ointments. Some people choose to combine multiple emollients, such as a cream and an ointment by putting the cream on throughout the day and ointment at night.
If you are using a cream, lotion or gel and your skin is still dry it is worth considering if you are applying regularly enough and if so, it might be worth trying a thicker preparation such as an ointment. We’ve put together an emollient guide below to help you choose the right emollient for you. This shows you the different types of emollients with the thinnest least moisturising lotions at the top and thickest most moisturising ointments at the bottom. The thinner lotions are good for people with mild psoriasis that is well controlled and just need a small amount of moisturiser to manage their symptoms, while the thicker ointments are useful for someone with extremely dry skin that is still dry after applying plenty of gels. See our guide below for more information about the various emollients we offer and find the best one for you.
Emollient Guide
Lighter less oily preparations
(Less moisturising)
Lotions: Aveeno Daily Moisturising Lotion, CeraVe AM Facial Moisturising Lotion, Cetraben Lotion, Dermol 500 Lotion.
Thicker more oily preparations
(More moisturising)
Ointments: Cetraben Ointment, Epaderm Ointment, Sebco Ointment.
Other preparations
Soap substitutes: Cetraben Bath Additive, Dermol 200 Shower Emollient, CeraVe Hydrating Cleanser.
Soap substitutes are useful if soaps trigger your psoriasis however they are washed off quickly so will not moisturise the skin very effectively.
Antimicrobial Creams: Dermol Cream, Dermol 200 Shower Emollient, Dermol 500 Lotion, Hibiscrub Antibacterial Skin Cleanser.
Antimicrobial creams are useful if your psoriasis is often getting infected or if you are using the cream as a soap substitute.
Antibiotic Creams: Fucidin Cream, Fucidin H Cream, Fucibet Cream, Betamethasone with Neomycin Cream, Betamethasone with Clioquinol cream.
Antibiotic containing creams should only be used where you are treating an active infection. They are for short-term use to treat the infection. Some of these also contain steroids to treat active flares of psoriasis at the same time. You should only use these if you have been told by a clinician your psoriasis is infected.
Salicylic Acid
Some psoriasis patients find their lesions can develop very thick scale. For this reason it is sometimes necessary to remove some of this scale before starting some of the treatments mentioned above. Salicylic acid can be useful in removing this scale and can be combined in certain products with a potent steroid (e.g.- Diprosalic) to help treat plaques with significant scale.
Coal Tar preparations such as Exorex lotion
These can be used long term and are particularly useful for large thin plaques. They can also be used in patients with many smaller plaques that are present over a large area of the body, where applying a steroid to each plaque individually would be challenging. Coal tar products are also safe to use on sensitive and thinner areas of skin.
Calcineurin Inhibitors
These are specialist creams reserved to treat certain types of difficult to treat psoriasis. They include the creams Elidel (pimecrolimus) and Protopic (tacrolimus). They work by affecting the immune system, blocking it from reacting and stopping psoriasis flares.
These creams are particularly useful in patients with psoriasis in areas of sensitive skin such as the face or genitals, or in those that have experienced significant negative side effects from steroid creams. These creams are relatively new but are not thought to have the same negative side effects associated with steroid creams, such as skin thinning or staining, so can be a better alternative in people that would otherwise require regular courses of steroids to treat psoriasis in sensitive areas of their skin.
These treatments are available here at DigiDerm but due to the specialist nature, we may need to speak to you, to make sure it’s the right treatment for you, if you haven’t had it from us before. If you think you might need one of these creams find out more information here
Tazarotene (Zorac 0.05% or 0.1% gel)
This is a retinoid medication. Retinoids are molecules related to vitamin A. They are often used in acne but this medication in particular can be used to treat mild to moderate plaque psoriasis. It is licensed to be applied to areas of up to 10% of the body so is not appropriate if your psoriasis is all over your body.
They are very dangerous for the baby if taken in pregnancy and for this reason pregnant women or those planning a pregnancy cannot use them and women of child bearing potential should use a reliable form of contraception if there is any chance of sexual activity whilst using the medication.
These creams can be used once daily for up to 12 weeks and work by slowing the overgrowth of skin cells and thus reducing the inflammation associated with psoriasis.
These creams can cause some skin irritation as a side effect such as burning, itching or stinging and for this reason are sometimes used with a steroid cream at the other end of the day to minimise irritation.
We do not currently offer this treatment so if you think it might be right for you we would recommend consulting with your GP or dermatologist.
Second Line Treatments
For patients that do not see benefit from the various applications mentioned above, second line options may be considered.
These include:
Phototherapy
Specialist dermatology centres can use certain types of ultraviolet light to help treat psoriasis. This is usually done with a form of light known as ultraviolet light B or UVB. UVB light slows the growth of the skin cells helping to reduce inflammation and when used on a regular schedule can successfully control psoriasis in certain people.
Ciclosporin
This medication suppresses the immune systems response and as a result improves psoriasis symptoms. It can affect the liver, kidney and immune system and for this reason requires regular blood tests to monitor. For this reason we are unable to prescribe this at DigiDerm. If you feel this medication might be right for you, it will need to be prescribed by a dermatologist so we would recommend contacting one or talking to your GP about the potential for a referral to dermatology.
Methotrexate
This is another medication that works by suppressing the immune systems response to help treat psoriasis. It is also used in psoriatic arthritis so may be beneficial if you also suffer with this. This is a highly effective medication for psoriasis but like ciclosporin above will require regular blood tests and thus cannot be prescribed here at DigiDerm so a dermatologist appointment will be needed if you want to discuss starting this medication.
Biologics and Biosimilars
Biologics and biosimilars are newer forms of medication used to treat psoriasis and psoriatic arthritis. They work by targeting specific stages of the autoimmune response, as opposed to some of the immunosuppressants mentioned above that weaken the whole immune response.
There is a lot of new evidence emerging around the use of these medications but at the moment the long term effects are not well known, so they tend to be reserved for use after first line and second line treatments have failed.
Much like the immunosuppressants mentioned above they will require regular blood monitoring and so would need to be prescribed by a specialist dermatologist.
Acitretin
This is a tablet form of retinoid (vitamin A type molecule). It works similarly to the cream form mentioned above (tazarotene) by reducing the overgrowth of skin cells and through this action helps to treat psoriasis.
This medicine is particularly useful for treating hand and foot psoriasis with significant thick plaques of hardened skin.
Make sure to moisturise regularly multiple times a day. If you have dry skin despite moisturising regularly. You may not be using the right moisturiser. Thicker ointment moisturisers are better at locking moisture into the skin than thinner creams and lotions. Consider switching to one of our ointments and this should improve things.
Use steroid creams when needed for flares but apply thinly and only for a maximum of 2 weeks at a time. 1 week is usually sufficient.
Try to identify triggers and avoid these wherever possible. This could be certain foods, soaps, clothing or detergents.
Small amounts of regular sunlight can help improve psoriasis symptoms but be careful not to get too much, as sunburn along with any trauma to the skin, can be a trigger for psoriasis. Too much sun can also increase your risk of skin cancers so make sure to keep the exposure limited and avoid midday sun.
Stress can cause psoriasis flares. It’s a busy life and sometimes stress can get on top of us. There is lots of help out there though, so try bringing down your stress levels and you may find this improves your psoriasis. Check out our mental health page for more information.

A Guide to Psoriasis
At DigiDerm we know how frustrating it is to suffer with skin conditions and how easy it is to get lost in all the information out there on the internet. We’ve put together this guide to give you all you need to know about psoriasis and most importantly how you can manage your psoriasis, and get back to doing the things you love, without it getting in the way!
DigiDerm is run by practicing NHS clinicians and we pride ourselves on providing you the best evidence based care. If you know what you need you can go straight to our treatments and select the treatment you want.
If you’re not sure what you need then we’ve put together some info below to help you find out more about psoriasis and what treatment is right for you. If you’re still not sure at the end then don’t hesitate to book a telephone or video consultation with one of our clinicians. We would be happy to help with any questions and if we can’t help, you won’t pay a penny. We’ll follow you up to check everything’s working as it should be and make sure you get the right treatments for your psoriasis.
Make sure to check out our FAQs section below, which has some of the most common questions we get about psoriasis.

What you need to know about Psoriasis
Psoriasis is a fairly common inflammatory condition of the skin affecting around 3% of the population. Recent research suggests that psoriasis is likely an autoimmune disease. This is a condition where the body’s own immune system attacks itself.
Psoriasis can start at any age but is most likely to present between the ages of 20 and 30 or 50 and 60. It can affect anyone and is equally likely to affect men and women but is more common amongst white people and less common amongst the Asian, black and Hispanic races. It tends to present as red and inflamed scaly plaques and most commonly appears on extensor areas of the skin. This means the areas of the skin that bend such as the front of the knees or backs of the elbows and can also commonly occur on the scalp. Whilst these are the most common presentations of psoriasis, symptoms can also be widespread covering large areas of the body.
Is Psoriasis linked to arthritis?
Put simply yes. This condition is commonly associated with a particular form of arthritis called psoriatic arthritis and studies suggest that up to 30% of people with psoriasis could have this form of arthritis.
Is psoriasis linked to Heart Disease?
Sadly this is another yes. Studies suggest a strong link between psoriasis and heart disease, although this is more common in people that have severe psoriasis. It is important to report any potential heart issues to your GP and even more important if you have psoriasis. Your GP will likely have a lower threshold for referring you for further tests. Potential signs of heart disease include: chest pain, shortness of breath, dizziness, blackouts, palpitations (feeling your heart flutter in your chest), etc.
If you have had any of the above symptoms we recommend contacting your GP for further advice.
What Causes Psoriasis?
Is Psoriasis Genetic?
There is thought to be a very strong link with genetics and the cause of psoriasis. Of the people that develop psoriasis, 40-50% of them are estimated to have another family member that suffers with the condition. This is even more likely to be the case if you first developed psoriasis before the age of 20.
What Triggers Psoriasis?
Stress is a well-documented trigger for psoriasis flares. If you are struggling with your stress levels then this is something worth looking at to get your psoriasis under control. At DigiDerm we understand how important stress and mental health are when it comes to skin conditions, so check out our mental health page for more information and resources that can help you.
Sunlight: Most people will find sunlight beneficial to their psoriasis and will actually find exposure to sunlight will settle their psoriasis however in a smaller number of people sunlight can make their condition worse.
Smoking is generally terrible for your health and so if you needed another reason to quit it’s also known to cause and worsen psoriasis. Not to mention it increases your risk of heart disease which having psoriasis already does. Stopping smoking is very difficult but with the right help it is absolutely possible. Talk to your local Chemist about how they can help you with this.
Trauma: Sometimes psoriasis can occur at the site of an injury to your skin. This is known as Koebner Phenomenon.
Drugs: A number of medications have been linked with psoriasis. Some of the most common examples include but are not limited to: lithium, imiquimod, terbinafine, beta blockers and drugs to treat malaria such as chloroquine.
If you think one of your medications has caused psoriasis, it is important you do not stop taking them but to speak to your GP or whoever prescribes it to you for more advice.
Pregnancy: Many women will find that their psoriasis actually improves during pregnancy. It can however get worse after giving birth.
Alcohol: Heavy drinking has been linked with psoriasis and it is thought that alcohol may have a direct impact in worsening psoriasis. If you feel you need help with cutting back on drinking then contact your GP or local drug and alcohol service.
Streptococcal infections: Streptococcus is a type of bacteria commonly associated with tonsillitis (Infection of the tonsils). Infections with this bacteria particularly of the throat are known to provoke a specific type of psoriasis known as guttate psoriasis. Guttate psoriasis causes small (generally less than 1cm) sores to appear often covering a large area of the body including the chest, arms, legs and scalp.
HIV: It’s important to be aware that severe or treatment resistant psoriasis has been identified as a recognised potential indicator of HIV and can be the first sign in some patients. If you think this is a possibility then its best to speak to your local sexual health clinic who can help you with getting tested and ruling this out.

What are the Symptoms of Psoriasis?
There are different types of psoriasis and it can appear in a variety of circumstances or areas, so the symptoms may differ depending on the type of psoriasis you are experiencing.
We will cover the most common types in this guide but there are some rarer forms as well. The main types of psoriasis are listed below with example images to demonstrate how it can present.
Plaque Psoriasis
This is the most common type of psoriasis and of the people that develop psoriasis 80-90% develop this type. Dry and scaly skin lesions known as plaques develop on the skin. These lesions can appear anywhere on the body but are most common on the elbows, knees, scalp and lower back. The plaques can be itchy and painful.
Scalp Psoriasis
This is a type of plaque psoriasis as mentioned above. It can appear in parts or over the whole scalp. Some people find it very itchy whilst others will experience no discomfort.
Nail Psoriasis
Nails are affected in around half of all people that suffer with psoriasis. It can cause the nails to develop dents or become discoloured. In some circumstances it can even cause nails to crumble or separate from the nail bed. You can use the same creams to treat nail psoriasis as with other forms of psoriasis however you may need to treat these longer than a flare on the skin, as nails can be difficult to treat. If using steroid creams potent or very potent steroids tend to be better suited for nail psoriasis. See our steroid guide for more info.
Guttate Psoriasis
This type of psoriasis has been shown to occur more commonly after sore throat infections caused by the bacteria streptococcus. It presents as small (less than 1cm) sores over large portions of the body, often including the chest, arms, legs and scalp. This condition is more likely to occur in younger people such as children and teenagers.
Inverse (Flexural) Psoriasis
This type of psoriasis effects the folds in the skin and areas of skin that regularly rub together. This is most likely to occur in the armpits, between the buttocks, under the breasts and around the groin. These are also common locations for eczema to occur so it is important to consider this and get a diagnosis from a healthcare professional before starting treatment.
How is Psoriasis Diagnosed?
Psoriasis is generally not too difficult for a clinician to diagnose. It has some typical features generally including red, inflamed, dry skin with a fairly characteristic silvery scale in most cases.
Whilst it is generally straight forward it can at times be unclear if its psoriasis or another skin condition, so if you are in any doubt after looking at the pictures above, please don’t hesitate to book for a telephone or video consultation with one of our dermatology Pharmacists and we’ll be more than happy to help you figure it out. Click here to make appointment
What is the Best Treatment for Psoriasis?
NOTE: Don’t worry if you are unsure of what treatments to select. You can start a simple online questionnaire-based consultation, attach some photos, and we will let you know if the treatment you have selected is safe and appropriate- if not, we will recommend an alternative. If you’d prefer to talk over the phone, you can book in for a telephone or video consultation with one of our friendly dermatology specialists and we can recommend suitable treatments and advice.
Here we will discuss some of the treatment choices that we offer for psoriasis in line with the latest clinical guidelines for dermatology in the UK. We will also discuss some alternative treatments towards the end that we don’t currently offer but are interesting to learn about (click on the products for more information and to start a consultation).
We will start with steroids. These are to be used when you have a flare of psoriasis. Make sure to apply them sparingly and usually for no longer than 7 days continuously unless advised by a clinician. They are a great way to settle down a flare of psoriasis but not a long term solution.
There are varying strengths of steroids from mild to very potent. If you already know what strength you need, as you’ve had it before, this is likely to work for you again. If you have not tried steroid creams before it is worth being cautious and starting with a milder steroid, only using potent steroids on the advice of a clinician.
You should be particularly careful when applying steroid creams to sensitive skin areas such as your face. You shouldn’t apply steroids to the face unless advised to do so by a clinician after assessment and you should never use anything more than moderate strength steroids in this area.
We are happy to have a look at some pictures or speak on a video or telephone call to advise on what strength we think you need if you’re unsure. Click here to book an appointment
Steroid Cream Guide
Mild Steroid Creams:
e.g- Hydrocortisone 1.0% ointment/cream
(Can be applied to the face on advice of a clinician)
Moderate Steroid Creams:
e.g- Eumovate (clobetasone butyrate 0.05%) cream and Betnovate RD (betamethasone valerate 0.025%)
(Can be applied to the face or genitals on advice of a clinician)
Potent Steroid Creams:
e.g- Betnovate (betamethasone valerate 0.1%)
Combination products with vitamin D analogues (psoriasis only):
Dovobet (betamethasone dipropionate 0.05% with calcipotriol 50mcgs/g)
Enstilar (betamethasone dipropionate 0.05% with calcipotriol 50mcgs/g)
Do NOT apply to the face or genitals.
Very Potent Cteroid Creams:
e.g- Dermovate (clobetasol propionate 0.05%)
Do NOT apply to the face or genitals.
Vitamin D Analogues
Vitamin D analogues have been shown to be very effective in treating psoriasis flares. These provide a potential alternative to steroids so are particularly useful if you struggle with side effects when using steroids such as skin thinning or staining. They can also be used long term if needed whilst steroids can only be used for limited courses.
Two examples of these creams include:
Dovonex (calcipotriol) Ointment: This can be used for psoriasis flares although should not be used on the face or genitals, as it can cause irritation.
Silikis (calcitriol) ointment: This has a similar effect to the above ointment however has the added benefit of being suitable for use on the genitals or face. For this reason the ointment is particularly useful for flares in these areas where potent steroid creams would be inappropriate.
In addition to products containing vitamin D analogues alone, we also offer combination products that also contain a steroid. These are particularly useful in difficult to treat psoriasis or where the individual products alone have not cleared the flare.
Examples of such products include:
Dovobet ointment/gel or Enstilar foam (calcipotriol and betamethasone).
Both of these products contain a strong steroid as well as a vitamin D analogue and for this reason attack the psoriasis flare in two separate ways.
Enstilar is particularly useful if your psoriasis covers a large area, as it comes as a foam spray making it easier to apply over a large area more quickly.
Emollients
The other major component of most psoriasis treatment is finding the right emollient for you. Emollients form a protective barrier on the skin and block moisture from escaping. This prevents the skin from drying out and makes it less likely to become irritated and inflamed, as can often happen in psoriasis.
It is important to apply plenty of emollient and to do so regularly. Thicker ointments last for around 12 hours whilst creams, lotions and gels only tend to last around 8 hours, meaning you would need to apply these thinner preparations at least three times a day and ointment twice a day for optimal results.
Ointments are better at locking in moisture because they are thicker and more oily however because of their oily texture some people don’t like applying these as much, as they can remain visible on the skin for longer after being applied and can stick to clothing and bedding, etc. Creams, lotions and gels are generally better tolerated due to them being thinner and thus more easily absorbed by the skin but because of this they will not moisturise the skin as affectively as ointments. Some people choose to combine multiple emollients, such as a cream and an ointment by putting the cream on throughout the day and ointment at night.
If you are using a cream, lotion or gel and your skin is still dry it is worth considering if you are applying regularly enough and if so, it might be worth trying a thicker preparation such as an ointment. We’ve put together an emollient guide below to help you choose the right emollient for you. This shows you the different types of emollients with the thinnest least moisturising lotions at the top and thickest most moisturising ointments at the bottom. The thinner lotions are good for people with mild psoriasis that is well controlled and just need a small amount of moisturiser to manage their symptoms, while the thicker ointments are useful for someone with extremely dry skin that is still dry after applying plenty of gels. See our guide below for more information about the various emollients we offer and find the best one for you.
Emollient Guide
Lighter less oily preparations
(Less moisturising)
Lotions: Aveeno Daily Moisturising Lotion, CeraVe AM Facial Moisturising Lotion, Cetraben Lotion, Dermol 500 Lotion.
Creams: Aveeno Cream, Aveeno Dermexa Cream, Balneum Cream, Balneum Plus Cream, CeraVe Moisturising Cream, CeraVe SA Smoothing Cream, Cetraben Cream, Cetraben Oatmeal Cream, Dermol Cream, Diprobase Cream, E45 Cream, E45 Dermatitis Cream, Epaderm Cream, Zerobase Cream
Gels: Adex Gel, Doublebase Dayleve Gel, Doublebase Gel.
Thicker more oily preparations
(More moisturising)
Ointments: Cetraben Ointment, Epaderm Ointment, Sebco Ointment.
Other preparations
Soap substitutes: Cetraben Bath Additive, Dermol 200 Shower Emollient, CeraVe Hydrating Cleanser.
Soap substitutes are useful if soaps trigger your psoriasis however they are washed off quickly so will not moisturise the skin very effectively.
Antimicrobial Creams: Dermol Cream, Dermol 200 Shower Emollient, Dermol 500 Lotion, Hibiscrub Antibacterial Skin Cleanser.
Antimicrobial creams are useful if your psoriasis is often getting infected or if you are using the cream as a soap substitute.
Antibiotic Creams: Fucidin Cream, Fucidin H Cream, Fucibet Cream, Betamethasone with Neomycin Cream, Betamethasone with Clioquinol cream.
Antibiotic containing creams should only be used where you are treating an active infection. They are for short-term use to treat the infection. Some of these also contain steroids to treat active flares of psoriasis at the same time. You should only use these if you have been told by a clinician your psoriasis is infected.

What Alternative Treatments are there for Psoriasis?
Salicylic Acid
Some psoriasis patients find their lesions can develop very thick scale. For this reason it is sometimes necessary to remove some of this scale before starting some of the treatments mentioned above. Salicylic acid can be useful in removing this scale and can be combined in certain products with a potent steroid (e.g.- Diprosalic) to help treat plaques with significant scale.
Coal Tar preparations such as Exorex lotion
These can be used long term and are particularly useful for large thin plaques. They can also be used in patients with many smaller plaques that are present over a large area of the body, where applying a steroid to each plaque individually would be challenging. Coal tar products are also safe to use on sensitive and thinner areas of skin.
Calcineurin Inhibitors
These are specialist creams reserved to treat certain types of difficult to treat psoriasis. They include the creams Elidel (pimecrolimus) and Protopic (tacrolimus). They work by affecting the immune system, blocking it from reacting and stopping psoriasis flares.
These creams are particularly useful in patients with psoriasis in areas of sensitive skin such as the face or genitals, or in those that have experienced significant negative side effects from steroid creams. These creams are relatively new but are not thought to have the same negative side effects associated with steroid creams, such as skin thinning or staining, so can be a better alternative in people that would otherwise require regular courses of steroids to treat psoriasis in sensitive areas of their skin.
These treatments are available here at DigiDerm but due to the specialist nature, we may need to speak to you, to make sure it’s the right treatment for you, if you haven’t had it from us before. If you think you might need one of these creams find out more information here
Tazarotene (Zorac 0.05% or 0.1% gel)
This is a retinoid medication. Retinoids are molecules related to vitamin A. They are often used in acne but this medication in particular can be used to treat mild to moderate plaque psoriasis. It is licensed to be applied to areas of up to 10% of the body so is not appropriate if your psoriasis is all over your body.
They are very dangerous for the baby if taken in pregnancy and for this reason pregnant women or those planning a pregnancy cannot use them and women of child bearing potential should use a reliable form of contraception if there is any chance of sexual activity whilst using the medication.
These creams can be used once daily for up to 12 weeks and work by slowing the overgrowth of skin cells and thus reducing the inflammation associated with psoriasis.
These creams can cause some skin irritation as a side effect such as burning, itching or stinging and for this reason are sometimes used with a steroid cream at the other end of the day to minimise irritation.
We do not currently offer this treatment so if you think it might be right for you we would recommend consulting with your GP or dermatologist.
Second Line Treatments
For patients that do not see benefit from the various applications mentioned above, second line options may be considered.
These include:
Phototherapy
Specialist dermatology centres can use certain types of ultraviolet light to help treat psoriasis. This is usually done with a form of light known as ultraviolet light B or UVB. UVB light slows the growth of the skin cells helping to reduce inflammation and when used on a regular schedule can successfully control psoriasis in certain people.
Ciclosporin
This medication suppresses the immune systems response and as a result improves psoriasis symptoms. It can affect the liver, kidney and immune system and for this reason requires regular blood tests to monitor. For this reason we are unable to prescribe this at DigiDerm. If you feel this medication might be right for you, it will need to be prescribed by a dermatologist so we would recommend contacting one or talking to your GP about the potential for a referral to dermatology.
Methotrexate
This is another medication that works by suppressing the immune systems response to help treat psoriasis. It is also used in psoriatic arthritis so may be beneficial if you also suffer with this. This is a highly effective medication for psoriasis but like ciclosporin above will require regular blood tests and thus cannot be prescribed here at DigiDerm so a dermatologist appointment will be needed if you want to discuss starting this medication.
Acitretin
This is a tablet form of retinoid (vitamin A type molecule). It works similarly to the cream form mentioned above (tazarotene) by reducing the overgrowth of skin cells and through this action helps to treat psoriasis.
This medicine is particularly useful for treating hand and foot psoriasis with significant thick plaques of hardened skin.
Biologics and Biosimilars
Biologics and biosimilars are newer forms of medication used to treat psoriasis and psoriatic arthritis. They work by targeting specific stages of the autoimmune response, as opposed to some of the immunosuppressants mentioned above that weaken the whole immune response.
There is a lot of new evidence emerging around the use of these medications but at the moment the long term effects are not well known, so they tend to be reserved for use after first line and second line treatments have failed.
Much like the immunosuppressants mentioned above they will require regular blood monitoring and so would need to be prescribed by a specialist dermatologist.
Top Tips for Psoriasis
Make sure to moisturise regularly multiple times a day. If you have dry skin despite moisturising regularly. You may not be using the right moisturiser. Thicker ointment moisturisers are better at locking moisture into the skin than thinner creams and lotions. Consider switching to one of our ointments and this should improve things.
Use steroid creams when needed for flares but apply thinly and only for a maximum of 2 weeks at a time. 1 week is usually sufficient.
Try to identify triggers and avoid these wherever possible. This could be certain foods, soaps, clothing or detergents.
Small amounts of regular sunlight can help improve psoriasis symptoms but be careful not to get too much, as sunburn along with any trauma to the skin, can be a trigger for psoriasis. Too much sun can also increase your risk of skin cancers so make sure to keep the exposure limited and avoid midday sun.
Stress can cause psoriasis flares. It’s a busy life and sometimes stress can get on top of us. There is lots of help out there though, so try bringing down your stress levels and you may find this improves your psoriasis. Check out our mental health page for more information.
Frequently Asked Questions
Frequently Asked Questions
Sadly there is no one treatment that is best. When using steroid creams, the preparation you use will largely depend on how severe your psoriasis is. You will hopefully have tried some of these creams already and will know if they have worked for you or not. If they have not worked for you, then there is a chance you may need to use a stronger steroid, additionally if you have only ever used steroid creams it may be worth trying a cream that contains both a steroid and a vitamin D analogue, as these can be particularly beneficial for treating psoriasis flares.
See our guide above titled ‘What is the Best Treatment for Psoriasis?’. This takes you through the various psoriasis creams available and discusses their potency, side effects, advantages and disadvantages to help you find the right treatment for you. When it comes to steroids, the best cream for you is the lowest potency steroid required to clear your flare up.
See our ‘steroid cream guide’ above to find out more about the strength of different steroid creams available. If you still aren’t sure which to use then we are happy to discuss further over a video/telephone call or look at some pictures. Make an appointment now
In terms of emollients, again there is no ‘best’ cream. The best cream is one that works for you. Ointments are the best at locking in moisture and this is because they are thicker than creams or lotions. If your skin is very dry, an ointment is probably best however due to their thickness they are sometimes not tolerated by everyone, as they can leave the skin visibly oily and stick to clothes. Creams and lotions are generally preferred as they are better absorbed by the skin and don’t leave as thick of a coating on the skin. Whilst creams and lotions are generally preferred cosmetically they are not as successful at moisturising the skin but might be better if you can use them more regularly. You can also try using a combination such as applying the ointment at night and cream throughout the day. See our emollient guide above for more details on the right emollient for you.
If only! It would be great if we could get rid of psoriasis entirely but sadly this is generally not the case unless there is a clear cause for the psoriasis. Generally speaking, psoriasis will come and go in flares throughout your life. Whilst it is generally not possible to completely cure psoriasis, with the right help, you can get it under control and stop it impacting your life.
Check out the images above for various examples of psoriasis and its different types in our ‘How is Psoriasis Diagnosed?’ Section.
Psoriasis can occur at any time in life but is most likely to present between the ages of 20 and 30 or 50 and 60. It is thought to be highly related to genetics, so it’s likely it wasn’t caused by anything you’ve done although it can be triggered by certain actions such as excessive alcohol consumption, smoking, trauma to the skin, and certain infections.
Although psoriasis and eczema are often confused and can at times look similar, these are different conditions and are not related.
Psoriasis is an autoimmune disease caused by the body’s immune system attacking normal tissues such as the skin. Psoriasis is also associated with inflammation in other parts of the body and can increase the risk of other conditions developing such as: Type 2 diabetes and cardiovascular disease.
Eczema is a group of seven different skin conditions that cause the skin to become itchy and inflamed however is doesn’t increase you risk of other chronic conditions the way psoriasis does.
They both can lead to dry, itchy and inflamed/painful skin however they tend to have different appearances making them fairly easy to distinguish.
Psoriasis tends to have a more defined border and a silvery/scaly appearance.
Eczema is more common in the creases of joints such as the knees and elbows. While psoriasis is more common in the areas that extend so the back of the elbow or front of your knees.

Psoriasis: The image above shows typical psoriasis. Note the defined border, silvery scaly appearance to the lesion and the location on the back of the elbow.

Eczema: The image above shows typical eczema. Note the lack of a clear border, the inflamed red appearance and location at the crease of the elbow.
Most moisturising creams/lotions/ointments are safe during pregnancy. You should always read the label to check for each cream but these do not tend to contain anything harmful for your baby.
Here are some examples of pregnancy safe emollients we stock: Doublebase gel; Dermol lotion; Epaderm Ointment, E45 Cream and many more.
Vitamin D analogue containing products such as Enstilar and Dovobet are generally avoided as there is insufficient data for their safety in pregnancy and breast feeding.
Steroid creams are generally considered safe to use during pregnancy however you should try to avoid using potent steroids during pregnancy, as there is more theoretical risk of the cream being absorbed into the blood stream. The lowest strength cream required to treat your psoriasis is best. If you are pregnant and requesting medication from us, make sure to make a note of this on your request so we can advise accordingly.
While these medications are safe when breastfeeding you should avoid applying to the breast directly before breastfeeding, to avoid the baby ingesting any cream.
Psoriasis is not contagious and does not spread from person to person. When you are having a psoriasis flare it can become larger and seem to spread for a variety of reasons. This can be caused by irritation due to itching and could also happen if the skin has become infected. If you are concerned about your psoriasis spreading try one of our treatments or book an appointment with one of our clinicians
Sadly there is no catch all cure for psoriasis however with the right creams and treatments lots of people can get their psoriasis under control and stop it impacting their lives. We’ve helped lots of people do this here at DigiDerm and would love to help you do the same.
